Dr. Amy Wesa, Director of Immuno-Oncology Research at Champions Oncology, recently presented a Taconic Biosciences' webinar to share her insights on leveraging murine systems toward establishing models that epitomize patient populations and enable predictive outcomes. This presentation described how Champions Oncology is complementing PDX models with incorporated human immune cells to drive the next generation of patient-derived models.
Following her presentation, Dr. Wesa addressed numerous questions from audience participants. We present the full webinar Q&A here.
 Watch the Taconic Biosciences' Webinar:
Watch the Taconic Biosciences' Webinar:
Following her presentation, Dr. Wesa addressed numerous questions from audience participants. We present the full webinar Q&A here.
Q: Do you have any recommendations for tumor models that would allow simultaneous T cell and NK cell immune responses?
Q: Can you comment on the percentage of NK cells that engraft in hIL-15 NOG and how that compares to what is seen in a healthy human?
Q: For the different types of humanized models described, do you need irradiation before engraftment? Under what circumstances would you recommend irradiation?
Q: Do you have experience using your acute myeloid leukemia (AML) patient-derived xenograft (PDX) models with immuno-oncology agents?
Q: Please comment on the AML PDX variability and how this variability can be addressed when planning a study.
Q: Have you evaluated PDX with different MHC I expression levels in the hIL-15 NOG NK cell-engrafted model? For example, are you seeing differences in basal NK killing depending on whether or not the tumors are expressing MHC class I?
Q: Are you able to engraft NK cells or other immune cells that have been genetically modified first by a third party and shipped to you?
Q: Can you comment on a typical quantity of AML cells you engraft per mouse or does it vary across the different AML models?
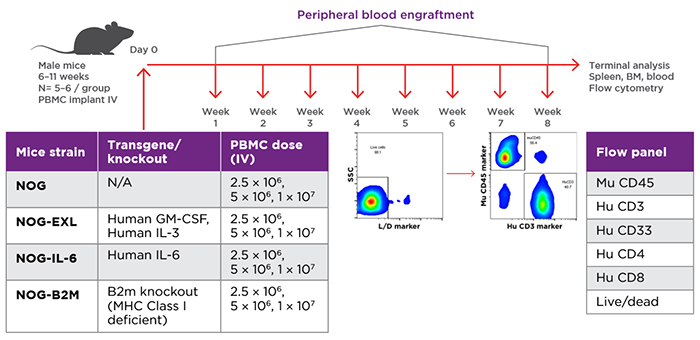
Study design for evaluation of PBMC engraftment in different NOG Portfolio strains. Source: Verma et al. 2019.
Q: Regarding use of expanded and fresh NK cells engrafted into hIL-15 NOG, do you already have banked NK cell inventory and can the cells be screened for particular properties prior to study?
Q: You presented a number of different humanized immune system mouse models for immuno-oncology. How do you select the appropriate model system? What is your guidance for the number of donors to use in a humanized immune system mouse study?
Q: Do you have NK cell or other (tumor-infiltrating lymphocyte) TIL information available for humanized mice studies?
