Metastatic Prostate Cancer Modeling with Humanized Mice
Taconic Biosciences
Tuesday, June 18th, 2019
Prostate cancer will likely remain among the leading causes of cancer-related deaths in men until improved therapies for advanced metastatic disease become available. According to Dr. Steve Kregel, a postdoctoral researcher working with Dr. Arul Chinnaiyan at the University of Michigan, a key barrier to improving prostate cancer therapies is the woefully inadequate models of metastatic disease used in preclinical drug testing.
At the 2019 American Association for Cancer Research (AACR) conference, Dr. Kregel presented work describing a new humanized mouse model of metastatic castration resistant prostate cancer that appears to overcome many of the limitations in its predecessors. To help us understand how his research could help improve preclinical prostate cancer modeling, Dr. Kregel responded to questions about the work he presented at AACR 2019.
Q: Why do you believe the commonly-used metastatic prostate cancer mouse models are inadequate?
“It's a big problem if the murine systems we rely on are unable to help us perform the research that needs to be done.”
–Dr. Kregel
Dr. Kregel: We can talk about current genetically engineered model (GEM) systems and human tumor xenograft models as two distinct systems, both having fundamental flaws for preclinical prostate cancer modeling.
GEM models of metastatic prostate cancer have three main flaws:
They rely on a mouse prostate that doesn't form sporadic tumors and differs anatomically and developmentally from the human prostate
They lack human-disease heterogeneity and rarely metastasize
Their disease progression is driven in a contrived manner unrelated to human disease and human disease drivers
With human xenograft models, the disease is inherently more human, but the model relies on tumor growth in an immunocompromised mouse. This means typical xenograft models can't be used for studying tumor-immune interactions and immunotherapy interventions. We know that tumor-immune interactions can have major impact on cancer biology, including on metastatic outgrowth and therapeutic response. Furthermore, the benefits of immunotherapies for treating cancer are real, but more avenues need to be explored. It's a big problem if the murine systems we rely on are unable to help us perform the research that needs to be done.
Q: What improvements are needed for prostate cancer modeling and how did you plan research to address the needed improvements?
Dr. Kregel: Prostate cancer researchers need a human-derived model that can recapitulate the natural history of the disease — from initiation to metastatic spread. It should also metastasize to clinically relevant locations like bone and needs to respond appropriately to standard of care [androgen receptor (AR)] targeted hormonal therapies. We also need to be able to model many distinct human prostate cancers, which xenograft modeling does permit, but we need an intact immune system too so we can model immunotherapy responses.
Our hypothesis was that humanizing tumor-immune interactions would improve modeling of metastatic prostate cancer, and perhaps improve modeling of hormonal and immune therapies. We generated a prostate cancer xenograft model in huNOG mice, which develop an intact human immune system from engrafted CD34+ stem cells, and we used this model to test our hypothesis.
Q: What was the approach used to evaluate your immune-humanized metastatic prostate cancer model?
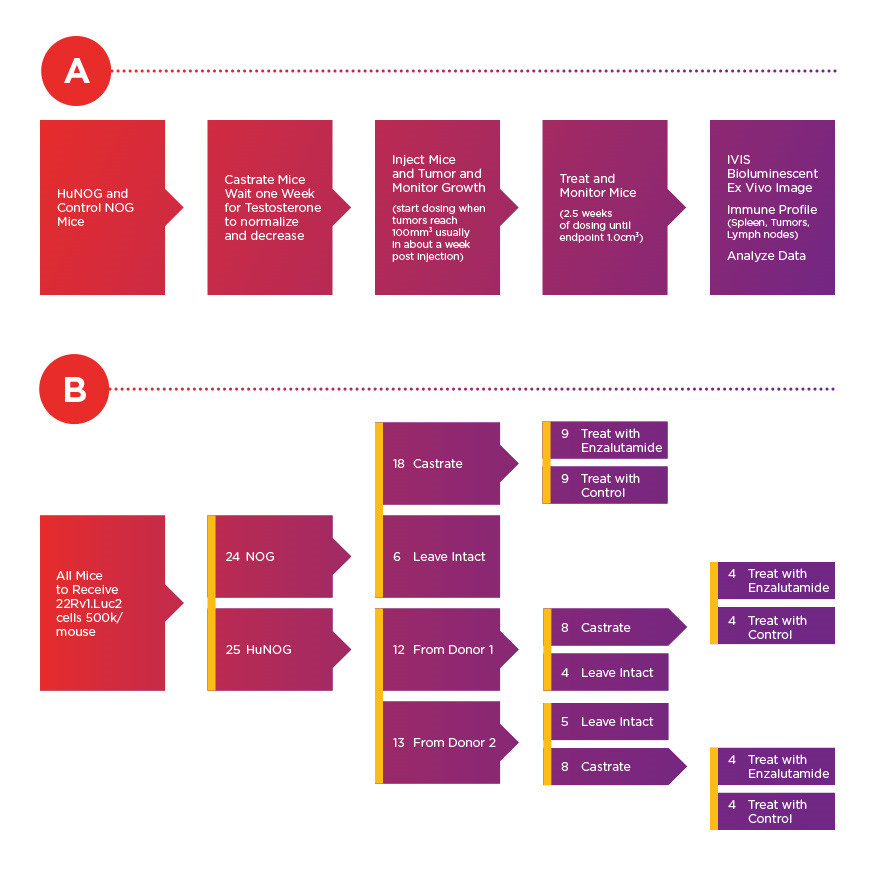
Dr. Kregel: We used conventional NOG mice and huNOG [CD34+ stem-cell engrafted NOG] mice as hosts for subcutaneous prostate cancer xenografts. After tumors had established, NOG and huNOG mice received either vehicle or enzalutamide [AR-targeted therapy], and we monitored tumor growth to the study endpoint.
The prostate cancer cells we used were engineered to express luciferase, which allows us to easily measure organ-specific metastatic growth at the end of the study. This design allowed us to observe how the presence or absence of a human immune system impacts growth at the primary-injection site, metastasis and metastatic outgrowth, and enzalutamide response.
Experimental timeline (A) and conditions (B) for assessment of 22Rv1.luc2 xenografts cells. According to Dr. Steve Kregel, 22Rv1 cells are among the most aggressive prostate cancer cell lines in vivo that still have androgen receptor expression.
Q: How would you summarize your key observations?
University of Michigan researchers observed a significant increase in the metastatic burden of NOG control mice castrated and treated with enzalutamide, and a significant decrease in metastatic outgrowth in enzalutamide-treated huNOG mice. Cancer cells were seen in the bone marrow and matrix of the epiphyseal head of a mouse femur (yellow arrow indicates 22Rv1 tumor mass). Femoral metastases were confirmed by histology (H&E stain) and a pathologist's assessment.
Dr. Kregel: Our key observations were related to metastasis, but it helps to contrast them with the observations at the primary tumor site across our experimental conditions. Comparing NOG and huNOG mice, regardless of treatment, primary tumor size was not significantly altered. However, the extent of metastasis and metastatic outgrowth at secondary sites was markedly reduced with enzalutamide treatment, but only in the huNOG mice with human immune systems.
We observed reduced metastatic growth following enzalutamide treatments in two different cohorts of huNOG mice, each produced with human stem cells from a different human donor. In a sense, each cohort acts as an avatar for the donor's immune system and for modeling how it might interact with prostate cancer. Our results align with recently published clinical data that suggests enzalutamide prevents metastatic growth in patients, and further suggest that anti-metastatic effects from enzalutamide could be mediated by the immune system.
Q: Were there any other notable observations from your work you can share?
Dr. Kregel: Previous data in our lab had shown that there was a seemingly paradoxical increase in the metastatic burden in immunodeficient mice treated with enzalutamide — presumably through the selection of resistant or aggressive metastatic clones. This effect is the opposite of enzalutamide's reported effects in the clinical data. The same paradoxical increase in the metastatic burden was seen in NOG mice, but not in either cohort of immune-humanized huNOG mice. Instead, the enzalutamide reduced metastatic burden, matching what is observed in the clinic.
Another interesting observation was increased T-cell infiltration in the tumors of the huNOG mice treated with enzalutamide when compared to hormonally intact or castrated mice. The T-cells infiltrating the tumors also expressed more interferon-γ, which is a read-out of their activation, and suggests that enzalutamide has the potential to help activate the immune system in patients. More work is needed to assess whether this is directly mediating the response seen with the decrease in metastases, or if the enzalutamide is acting directly on the immune cells, or if the mechanism is more complicated through tumor- and immune-cell cross talk.
Q: What are you next steps for this system?
Dr. Kregel: The clearest next steps are to further characterize the model in other cell lines and with human patient derived xenograft samples, and of course test an immunotherapy such as an immune checkpoint inhibitor like anti-PD-1 treatment. We would also like to really tease apart the mechanism of how enzalutamide and AR-antagonism in the immune cells helps prevent metastatic outgrowth.
There are numerous other approaches I'd like to apply and study with these models, including the huNOG-EXL model and similar hosts expressing human cytokines for better human myeloid cell engraftment. For example, we currently have focused a lot on the lymphoid activation, but if we want to investigate novel therapies, such as STING agonists, or how radiation and chemotherapy impact immune activation in prostate cancer, huNOG-EXL or other models that are better at engrafting human myeloid cells might be necessary.
Q: How do you see this model impacting preclinical prostate cancer research?
“I believe this model has large potential for impacting the prostate cancer research field and could influence how we model everything in vivo to study prostate cancer.”
–Dr. Kregel
Dr. Kregel: I believe this model has large potential for impacting the prostate cancer research field and could influence how we model everything in vivo to study prostate cancer. Immunotherapy appears to be headed towards becoming the standard of care for many cancers, and few researchers have been testing therapies on human cancer with an intact immune system, let alone a model that has a human immune system and metastasizes to clinically relevant locations.
These models should be adaptable to nearly any human tumor and can model heterogeneity and response to the current standard of care AR-targeted therapies. GEM models clearly cannot do all of that. For researchers developing therapeutics for metastatic castration resistant prostate cancer, our system and approach is immediately worth considering adopting. Future work might lead to this type of approach becoming the gold standard for certain pre-clinical in vivo modeling.
Taconic Biosciences' model generation team has produced about 5,000 models in the last 15 years, developing a globally-recognized reputation for advancing the work of in vivo researchers. Our scientific program managers are here to help you navigate the complexities of model generation.
. Femoral metastases were confirmed by histology (H&E stain) and a pathologist's assessment.")

